
By Emily Boring
A golden rule: Never use the language of an eating disorder to talk back to an eating disorder.
Perhaps this sounds obvious. Unfortunately, I’ve found that in real-life situations—conversations with well-meaning clinicians, family, friends, and other recovery supporters—this rule is far from universally enacted or understood.
Here’s a classic example. On the day I was diagnosed with anorexia, I showed up in a dietitian’s office, paralyzed at the idea of eating more or restoring weight. “Don’t worry,” she assured me. “You can recover from anorexia and still be very thin.” (Cue forehead slap and groan).
Other statements are equally fatphobic and counterfactual, but a little more subtle. Recently, I shared my discomfort about my post-treatment body with a clinician. Knowing nothing about my weight or my medical condition, she said, “Well, sometimes bodies look different in the earliest stages of recovery. You may not have to stay in this body forever—later on, if you want, you can go back to more exercise.”
Or consider the scenarios I often encounter in the company of kind but unaware friends. Over lunch or snack, I’ll sometimes sigh about my meal plan or complain about having to eat six times a day. Frequently, someone says, “Yeah, that sounds really overwhelming. I mean, that’s an unnatural amount of food!”
What do all these statements have in common? In one way or another, they all employ the language and logic of an eating disorder to talk back to the anxiety caused by one! They’re all founded on beliefs like, “Thin = better,” “Fitness is a universal value,” or “Some amounts of food are ‘normal,’ and others are not.” In each case, the language is clearly chosen to comfort or reassure me—which doesn’t undo the harm.
For years, I attributed comments like these to fatphobia, diet culture, and sheer lack of information. And it’s true: weight stigma in medicine, science, and society is a rampant problem that leads to missed diagnoses, medical complications, lack of access to treatment, identity-based discrimination, and profound emotional pain. Doctors, dietitians, and therapists can complete entire degree programs with zero hours of training in eating disorders. But over the years, I’ve heard these comments again and again from well-educated, well-meaning people. And I began to think there’s something more at play.
Beneath each of these misguided statements, I hear the desire to extend empathy: the intention to meet me exactly where I am in recovery, providing comfort and companionship in the struggle. I hear a person longing to say, “I see you. I acknowledge your suffering. I’ll go there with you, because I want to help.”
I know this is true because I’ve been on both sides of these conversations. I remember times when I’ve sat beside a mentee or friend who’s paralyzed with discomfort and self-hatred. “I can’t stand my new body,” she’ll tell me. “It’s changed so much! I’ll never accept my recovered weight.” I know better, and yet I’m still tempted to use the language of the eating disorder—to say, “Don’t worry! The change isn’t nearly as drastic as you think it is. You’re beautiful and healthy; that’s what others see.”
In other words, I see a person I care for who’s suffering, unable to glimpse her radiance and potential, and all I want to do is to fix it and help! This impulse to stop the pain at any cost—an impulse shared by providers, family, friends, and more—is instinctual and well-meaning and strong.
But because I’ve had an eating disorder, I check myself before I use that kind of language. Given the reality of body dysmorphia, people recovering from eating disorders can’t see themselves clearly and usually overestimate physical changes. But I know that emphasizing outer appearance, even when you’re trying to be reassuring, only fortifies the belief that appearance dictates value. Downplaying physical changes might feel relieving in the moment. But it only strengthens the myth that larger bodies are unacceptable and change = bad.
Which brings me back to my rule: Never use the language of an eating disorder to talk back to one. Any short-term comfort that arises from doing so is outweighed by the profound long-term costs. In the following sections, I explain why speaking the language of the eating disorder is not a solution, and what you might say instead.
All-Or-Nothing Valleys: Why Eating Disorder Language Doesn’t Work
In a previous article, I wrote about the valley of the eating disorder and the valley of recovery. I used a simple drawing—a ball-and-cup diagram—to show that “recovery” and “illness” are two separate, self-sustaining locations, each with a distinct set of beliefs, experiences, and rules.
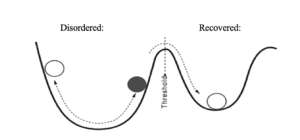
The starkness of this physical diagram highlights a crucial feature of eating disorders: these illnesses are all-or-nothing. From the valley of anorexia (a place of fear and rigidity), I can’t remember or envision the feelings in the valley of recovery (a place of freedom, trust, and ease). Anorexia’s rules feel natural, obvious, and logically consistent—ironclad in my mind, and reinforced by physical cues. This isn’t a failure of will or imagination. It’s a fact of biology, a product of the measurable metabolic and psychological changes that occur in the body and brain of someone with an eating disorder when they fall into energy deficit.
What this means is that everything you say to someone with an eating disorder gets processed through a highly selective, single-minded filter. It passes through a membrane that admits only the evidence that supports the eating disorder’s preexisting ideas. Or, the eating disorder alters the evidence carefully, twisting your words for its own ends. The only messages that have a prayer of escaping this insidious cycle are those that are equally insistent in the opposite direction: statements that speak, loudly and unequivocally, of a recovered worldview.
Here’s a way of illustrating it. I find it useful to observe not just what my eating disorder does with extremely fatphobic statements, but also how it responds to neutral or slightly ambiguous situations.
This comes up most often in discussions of my meal plan. At the outset of our work together, a dietitian usually gives me firm instructions, saying, “Here are the portions and times that your body needs to eat each day, and here’s what exercise can look like.” I don’t particularly like it (who, with anorexia, would?), and so I struggle to meet 100% of the goals. But strong instructions are also helpful. The ultimatum that “Food is medicine, and medicine is not optional” is one of the only messages powerful enough to cut through anorexia’s objections and let me start eating.
But as weeks pass and I leave out a snack here or cut corners there, succumbing to the whispers of my eating disorder, a dietitian will often change her strategy.
“I see you’re struggling to meet your meal plan,” she’ll say. “Day after day, you never add the snack you’re supposed to add for exercise. Why don’t we put a pause on that snack goal, and focus on the bare minimum? That way you won’t feel so overwhelmed.”
Her intention: To meet me where I am, setting goals that feel doable. To not let the futility of meeting a huge goal discourage me from taking the vital first steps.
What does my eating disorder hear? “If this snack is now optional, then why did she assign it in the first place? There must have been no reason! Clearly, this whole meal plan is suspect. Clearly, my body doesn’t need this energy. My weight must be high enough that it doesn’t matter if I eat at all!”
What I really needed to hear was unyielding, unwavering permission to follow my meal plan fully, no exceptions and no bargaining. I needed my dietitian to stand firm in her original message—as certain, in her insistence that I eat, as my eating disorder is about not eating. Otherwise, anorexia takes any wavering or compromise as license to obey its own rules.
This reaction isn’t unique to me. I’ll often describe these conversations to friends I met in treatment—people whose minds work in the same strange but systematic way. We all cringe and sigh at exactly the same moments. “Let me guess—your eating disorder heard it this way,” someone will say, and proceed to fill in (often nearly verbatim) every distorted thought my own brain produced.
In other words, the logic of an eating disorder may be biologically unnatural and unfounded in reality, but it’s not unpredictable. Its consistency is uncanny. Without fail, an eating disorder takes the tiniest shred of uncertainty, processes it through its own pre-formed convictions, and churns out the belief that you’re not sick enough, your body is unacceptable, and you don’t need to eat.
That’s why it never makes sense to speak the language of an eating disorder! When you’re trapped in the valley of illness, the thoughts that keep you there are devastating enough on their own. Now imagine that you hear, from someone who’s supposed to be helping you recover, a statement that endorses the very rules that operate in that valley! You’ll conclude exactly what the eating disorder is already saying: this diminished life is the only option. There must not be a place called “recovery.” The rules of my eating disorder are true.
And this is the crux of the problem. You—and now I mean family and friends and clinicians, everyone supporting recovery—can clearly see that there are two sides to the hill-and-valley diagram. You use the language of the eating disorder because you know there’s a world beyond illness, and you desperately want your loved one to see it, too. So you throw them a lifeline—a lifeline made of the language of thinness and fitness, the only words that someone with an eating disorder seems to be able to hear.
But in the valley of illness, we can’t see the recovered valley! For all we know, there’s nothing else out there. That’s how convincing and all-encompassing the lived experience of an eating disorder really is. So when you use disordered language, we don’t hear someone standing on the other side of the hill, coaxing us forward. We hear someone standing with us in the valley of illness, confirming that this is the right (and the only) place to be!
True empathy for someone with an eating disorder, then, looks different than you might expect it to. “Meeting us where we are” doesn’t mean joining us in the valley of illness, adopting its rules and vocabulary. It means reminding us that there are two sides to the diagram. It means standing in the other valley. It means showing, through words and actions, that there’s a place called “recovery” where the rules are radically different, and reminding us that with help, we can get there, too.
Here’s a secret: deep down, your client or friend or child is longing to hear this message. Even in the worst of my illness—moments when, to an outside observer, I seemed to want to be left alone with my anorexia and allowed to stay there—I was desperate for rescue. The first day I entered a dietitian’s office, I was outwardly defiant. My anxiety appeared as a vehement refusal to gain weight. But just below the surface, I was frightened and exhausted. I was terrified of this thing that had taken away my joy and my agency, making my world a miserable, hollow place. Beneath my resistance and protests, beneath my clinging to anorexia’s behaviors, I wanted nothing more than permission to let it all go. I yearned to hear someone say, “You don’t have to do this anymore. Lay down your burden. There’s another way to live.”
And when I didn’t receive this message—when instead the dietitian endorsed my desire for thinness, affirming my fears about my body—that tiny flame of hope was promptly extinguished. When you have an eating disorder, the seeds of resistance are extremely fragile. They’re vulnerable to the slightest discouragement, the subtlest external sign that confirms your illness must be “right.”
To support someone in recovery, you must be incredibly observant, careful, and patient. Often (indeed, usually), you won’t be able to see the desire for freedom that’s growing, quietly and cautiously, beneath the disordered behaviors. Usually you’ll see the opposite: a person who seems to cling, as if his or her life depended on it, to the worldview of their illness. It’s one of the cruelest ironies of an eating disorder: the illness’s surface manifestation obscures and contradicts the truths that are present, just underneath, longing to be acknowledged. So at any given moment, you—the supporter of recovery—must be ready. Ready to offer a unified, unequivocal invitation from the valley of recovery, so that when we finally feel strong enough (or weary enough) to receive it, the truth we need to be free is already there.
What “Equal and Opposite” Sounds Like: Tips for Recovery Conversations
The good news is this. Because of the eating disorder’s impressive predictability—because of how strongly and swiftly it skews every bit of evidence to support its underlying beliefs—it’s actually reasonably simple to counter. “Equal and opposite messaging” isn’t a mystery, and it isn’t something you have to invent anew every time. There are patterns you can learn—statements to offer, and statements to avoid—to guide nearly every conversation. Here are some of mine.
Think (and Imagine!) Before You Speak
Before I talk to someone with an eating disorder, I ask myself: How would a malnourished brain interpret this? When I was deep in my own illness, how might I have heard these words?
If you haven’t experienced an eating disorder, here are some questions to help you get started.
- Does this statement imply that some bodies are “better” than others?
- Does it suggest that some foods have greater (or lesser) moral worth?
- Does it uphold “health” (read: able-bodied fitness) as an unquestioned value?
- Does it include mention of numbers or behaviors that may be triggering?
- Could someone with an eating disorder use this statement as an excuse to restrict food or over exercise?
- Does this statement perpetuate the ideals of diet culture? Weight stigma?
- Does it emphasize physical traits over internal ones?
- Does it encourage comparison between people, in either a positive or negative way?
Remember: the person you’re speaking to will listen through a selective filter. If you answered “maybe” to any of these questions, then assume that the answer is “yes” for someone with an eating disorder, and reconsider your words.
Choose Questions, Not Announcements
The thing that makes me feel most unseen in recovery is this: when people try to guess my inner state based on outward appearance or actions. In recovery, external progress does not necessarily signify or produce inner wellbeing. In fact, the opposite is usually true for some time.
Rather than saying, “You ate your whole meal plan! You’re doing so well!”
Try saying, “I noticed you made progress in relation to the goals we set last week. How is that feeling for you? What’s going on in your head?”
Rather than, “You under-ate today, so you must be relapsing!”
Try, “I notice you avoided a food group at lunch. What went into that decision? Can I support you in any way?”
The eating disorder already believes in a strong link between emotion and behavior. Restricting can be an unconscious signal of suffering, a way to affirm, to yourself and others, that things feel “wrong” inside. Help us practice other ways to express our feelings—namely, by sharing them openly and directly. Teach us to trust that when we speak our inner truth, others will listen. We won’t be alone.
Provide Firm Boundaries, and Stick to Them
Remember what the eating disorder does with ambiguity. You—and here I especially mean clinicians—may think that giving someone choices about recovery is useful and respectful. You may think it’s a way to increase buy-in and involve patients as partners in care. But remember that at any given moment, you may be talking to two different “people”—the self of the eating disorder, and the healthy self. The eating disorder almost always has the louder voice. “Listening” to someone in recovery, then, all too often means giving airtime and credence to the eating disorder’s opinions, thereby failing to help the healthy self to learn how to speak.
So instead of open-ended choices or discussions, offer options within nonnegotiable boundaries.
Rather than asking, “What do you think should be our strategy around exercise this week?”
Say, “It’s not okay to use running as a way to cause energy deficit. This week, do you want to stop running altogether, or choose one short run with an extra snack?”
Instead of asking the person in recovery to help find motivation and vision (qualities that, in the valley of the eating disorder, are nearly impossible to access), provide a firm picture of “how it’s gonna be.”
Don’t say, “Surely you don’t want to relapse. Why don’t you make a list of the qualities of full recovery, and identify what’s holding you back?”
Say, “It’s not an option to keep restricting and over exercising like you have been. We’re going to turn this relapse around together. How do you want to make that happen—here, or in a higher level of care?”
I’ve met many providers who hesitate to use such strong language for fear of provoking rebellion or scaring us away. They worry that setting firm boundaries will be seen as the opposite of empathy—a sign of unwillingness to work with the fears we feel or respect the priorities we hold.
That’s not how I see it. Throughout recovery, I’ve learned that when a provider pushes back—when they insist that “I know best, and this is how we’re going to do things”—that’s a form of deep listening, a respect for my truest self. When my own motivation wanes, I can trust that others won’t let my recovery slide backward. If you have an eating disorder, the act of giving up choice is, paradoxically, the most powerful form of agency. By surrendering decisions about micro-level actions (what to eat, how to exercise) to my providers, I slowly took authority away from my eating disorder. I lost control over daily choices, yes, but I gained the choice of assenting to life.
What Do You Need? Claiming Your Recovery Messages
What I’ve described above won’t work for everyone. As a thin, white, cis-gendered female, I’ve been conditioned to follow rules and rewarded for doing so. I tend to respond to boundaries positively, using them to strengthen my healthy self’s voice. People of other identities—people whose bodies don’t benefit from systems of privilege and the rules that maintain them—may respond very differently and react to boundaries with resistance or distrust. I’m also young and able-bodied, determined to push through to the fullest recovery as swiftly as possible. I’ve met others who are weary from decades of struggle or co-occurring conditions, who need providers to say, “Let’s take this slowly, as you feel comfortable. You’re in charge.” By definition, empathy looks different for every individual. Personal reflection—what works and what doesn’t, for you—is the most powerful tool.
To you in recovery, then, I invite you to think back to a time when you did feel supported. Maybe you walked out of a dietitian’s office feeling motivated and encouraged, suddenly clear about what you had to do that week. Maybe you talked about the struggle of recovering with a friend and felt validated and heard. Among these encounters, can you notice any patterns or similarities? Are you a person who responds to negative or positive reinforcement? Do you need directness, or gentleness? Affirmation, or tough love? Once you’ve identified what works, consider telling your supporters: “I understand why you’ve been doing/saying things like you have, but here’s how my eating disorder hears it. Could we try this instead?”
As a friend of mine wisely put it, relationships with the people who support you in recovery are like any relationship: they require feedback and communication. You wouldn’t expect a best friend or partner to intuitively guess your love language. Instead, you tell them what you need and want, recognizing that doing so will benefit both of you. So, too, with clinicians and friends and family. Recovery is confusing and difficult for everyone. Why not make it simpler by asking for what you need?
In case you need help getting started, these are the messages I’m most often craving—the things I can’t hear enough of when recovery feels futile and exhausting.
I know it’s hard.
I see the work you’re doing.
Your feelings are valid.
You’re enough.
I promise it gets better, and I know you can’t see that right now.
If you make mistakes, I’m here to catch you.
You’re not alone.
You’re never beyond hope or help.
These are messages that most people long for. They’re reminders of connection and worthiness, which are basic desires of all human beings. If we go too long without hearing these messages, we turn to misguided methods, behaviors that cunningly promise to meet our needs but leave us empty and bare. For me, the misguided methods are an eating disorder, and the antidote is true companionship—companionship that acknowledges where I am, but which also reminds me of the place I’m going. I need companionship that can turn an isolating illness into a reminder of the needs we all share.
Emily Boring is a writer and scientist from Corvallis, Oregon. A graduate of Yale University (’18), she earned her Masters of Science (’20) in marine ecology and genetics at Oregon State. Since recovering from anorexia nervosa during college, she has become an active speaker, writer, and one-on-one mentor. Her writing has appeared on the F.E.A.S.T. blog, Recovery Warriors and The Mighty. She is currently pursuing her Master’s of Divinity at Yale, focusing especially on religion and literature. She hopes to write and teach at the intersection of science and spirituality, using this shared language to help others through processes of healing. You can reach her at emilylauraboring@gmail.com.
5 Responses
Great read! Hope to see more like this. It is hard to know how to support a loved one battling this terrible disorder. Thank you for sharing.
Thank you for this great article! As a supporter of my 19 yo daughter in recovery, it’s so daunting to see her making huge strides but knowing that outside of her program is still the world obsessed with diets, thin and the ever-morphing “healthy”. I really appreciate the language and tactics you offer.
I feel the same way. This is a fantastic article and I wish I had found it a year and a half ago. I’m supporting my 17 year old daughter in her recovery and hoping to help her to be ready for college. I have said things in the past that I now realize left the door way open for my daughter’s anorexia to rush in, allowing her to remain in the valley of illness. I am going to write down phrases from this article so I can refer to them and get guidance and strength and also a sense of hope.
Thank you Emily.
Just what I needed to read early this morning when awake with anxiety over my 29 yr old daughter’s relapse with anorexia. Thank you for your very insightful, helpful post, Emily.
This is really eye-opening. Thank you so much for sharing, Emily!